
Teachers’ Perception On COVID-19 Vaccine: Implications on COVID-19 Prevention in Kenya
Patrick M. Mutua1*, Joshua M. Mutiso2, Jemimah A. Simabuni2, Michael M. Gicheru2
1ImmunoBiologic Research and Consultancy Centre, P.O Box 295, Kibwezi, Kenya
2Department of Zoological Sciences, Kenyatta University, P.O Box 30709-00100, Nairobi, Kenya
Abstract
Currently, there are 89 coronavirus disease 2019 (COVID-19) vaccines in different phases of clinical trials. Twelve COVID-19 vaccines have been approved for emergency use in different countries. The Kenyan government has approved Oxford-AstraZeneca COVID-19 vaccine and is in the process of rolling out vaccination to priority targeted groups based on the World Health Organization (WHO) roadmap for prioritizing uses of COVID-19 vaccines in the context of limited supply. Among the targeted priority groups by the Kenyan government are teachers. In January, 2021, we surveyed 380 teachers in Kinango and Samburu sub counties in Kwale county in Coast region in Kenya to determine knowledge gaps, opportunities, acceptance rates and factors influencing acceptance of COVID-19 vaccine. ANOVA followed by Tukeys Post Hoc analyses were performed to determine the effect of gender and level of education on COVID-19 vaccine potential acceptance and in evaluating the effect of teaching experience and teachers age on vaccine safety. While 99.5 % of the respondents knew COVID-19 is a viral disease and were able to list three correct symptoms of the infection and that 41.1 % knew of a person who had died of COVID-19, only 34.7 % agreed they would accept to be vaccinated if the vaccine was safe. Male and female teachers with primary teacher certificate and diploma qualifications were more likely (PË0.05) to accept to be vaccinated compared to teachers holding degrees. However, the association between vaccine acceptance among the certificate and diploma respondents was not (PË0.05) significant. Additionally, 36.8 % of the sampled teachers knew they are targeted priority group for the COVID-19 vaccination with 92.4 % of the teachers agreeing that they needed more information on the vaccine. Among the sampled, only 12.9 % thought the vaccine was safe. Teachers aged 23-35 years and those aged 46-59 years comprising of 11.5 % and 56.1% respectively of the sampled teachers, substantially (PË0.05) disagreed the vaccine was safe compared to teachers aged 36-45 years who formed 8.7 % of the sampled respondents. Among the interviewees, 93.1 % suggested a joint approach by the Teachers Service Commission (TSC) and Ministry of Education (MoE) in leading the COVID-19 vaccine campaign awareness. Based on these data, there is need by the government, particularly the TSC and MoE and other public health providers, to mount serious public vaccination literacy campaign in order to promote trust among Kenyan teachers and bolster voluntary COVID-19 vaccine uptake. Further, the government should seize the high COVID-19 vaccine acceptance potential among primary certificate and diploma teachers in prioritizing COVID-19 vaccine roll out among teachers. Primary school teachers should, based on WHO roadmap of sequential distribution of the vaccines, be vaccinated before the secondary school teachers because of inability to effectively keep physically distant form their learners and also due to high congestion in the institutions.
Introduction
The World Health Organization (WHO) Strategic Advisory Group of Experts on immunization defined vaccine hesitancy as a delay in acceptance or refusal of vaccination despite availability of vaccination services. Vaccine hesitancy varies in intensity and form depending on when and where it occurs and what vaccine is involved1,2. The WHO identified vaccine hesitancy as one of the top ten global health threats in 2019 (https:/www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019). A study in Kenya observed insufficient public education surrounding vaccination, inadequate training for health caregivers on immunization, persistent challenge of stock-outs of vaccines and vaccination-related supplies and an emerging strong anti-vaccination movement that has been spreading misinformation regarding vaccine safety using social media and other platform as some of the main causes of vaccine hesitancy in the country3. Vaccine hesitancy in Kenya presents substantial obstacles to achieving coverage and herd immunity4,5. The Kenyan government, through the Ministry of Health, approved Oxford-AstraZeneca COVID-19 vaccine through the African Union initiative for use to vaccinate targeted groups6. On 31st of December, 2019, the WHO was informed of an outbreak of cluster of pneumonia cases in the Wuhan City, Hubei Province in China. This was subsequently confirmed as an outbreak of a new type of coronavirus disease 2019 abbreviated COVID-197. The Kenyan basic education sector was impacted negatively by outbreak of COVID-19 pandemic. Among the identified adverse effects of COVID-19 on Kenyan education sector included widened physical contact between the teachers and learners as a result of prolonged school closures, cessation of public library services, economic shocks spillover to underprivileged learners’ families, unequal access to digital educational resources and materials and upsurge of anti-social behaviors by learners8. The Ministry of Education (MoE) issued emergency response plan to mitigate the adverse effects imposed on the sector by COVID-19 which included opening of schools on 4th of January, 2021 after the institutions were closed on 16th March 2020. The report, however, identified congestion of pupils in schools, inadequate supply of water and sanitization facilities and masks as serious constrains in meeting Ministry of Health COVID-19 protocols in the institutions9. By 9th of February, 2021, Kenya had recorded 101,944 COVID-19 cases and 1786 deaths10. According to the Corona Vaccine Tracker, by 6th of February 2021, there were 12 COVID-19 vaccines that had been approved for emergency use in various countries in the world11. The WHO Strategic Advisory Group of Experts (SAGE) on Immunization developed a roadmap for prioritizing uses of COVID-19 vaccines in the context of limited supply12. Based on the SAGE roadmap, Kenya has prioritized teachers in public and private schools for vaccination as a long term strategic intervention in mitigating transmission of COVID-19 infections in schools and in the communities. The roadmap identifies teachers as belonging to social and employment groups at elevated risk of acquiring and transmitting COVID-19 infection because they are unable to effectively physically distance12. Despite the initiative to roll out massive vaccination of teachers, there is no report existing to guide the government on policy formulation and implementation so as to ensure successful vaccination of teachers against COVID-19. We present findings from a survey that sought to gather information regarding teachers’ knowledge on COVID-19 and COVID-19 vaccine as well as identification of challenges, factors and opportunities that may influence the vaccine acceptability among teachers in Kenya.
Results
The survey respondents represented a random sample of teachers in Kinango and Samburu sub counties in Kwale County, Kenya. The sub counties have total of 864 teachers spread across secondary and primary public schools. A total of 380 teachers, representing 44 % of the teachers’ population in the sub counties, were randomly selected and asked to fill a questionnaire with questions on COVID-19 and COVID vaccine so as to determine their level of awareness on the disease, the vaccine and to identify the teachers’ acceptability for COVID-19 vaccination. Of the 380 teachers, 127 were females while 253 were males. Their age ranged from 23 years to 59 years with a median age of 40 years. Among the interviewees, 157 had certificate of primary teaching as the highest level of education while 128 had diploma in education and 95 had degree. Teachers with five years of teaching experience were 105 and their age ranged from 23 years to 35 years, those whose teaching experience of 5 years to 10 years were 62 aged between 36 years to 45 and a total of 213 teachers aged between 46 years and 59 years had teaching experience spanning between 10 years to 20 years and more.
Table 1: Demographic characteristics of study respondents
|
Characteristic |
Frequency |
|
n |
380 (100 %) |
|
Female |
127 (33.4 %) |
|
Male |
253(66.6%) |
|
Teaching experience (Years) |
Number of respondents |
|
0-5 |
27.6 % |
|
6-10 |
28.2 % |
|
11-20 |
27.9 % |
|
Ë20 |
16.3 % |
|
Level of education |
Number of respondents |
|
Primary teacher certificate |
41.3 % |
|
Diploma in education |
33.7 % |
|
Degree |
25 % |
Table 1 shows a summary of the respondents’ demographic characteristics. When asked whether they knew the cause and three symptoms of COVID-19, 99.5 % of the interviewees said COVID-19 was a viral disease and were able to list three correct symptoms with high body temperature, dry cough and difficulties in breathing being the commonly listed symptoms. Only 21 % of the 378 respondents listed anosmia and dysgeusia as additional symptoms of the disease. Asked if they knew of a person known to them who had died of COVID-19, 41 % of the respondents responded in the affirmative. A total of 334 of the sampled teachers knew of existence of a COVID-19 test but only 8.2 % confirmed to have been tested as a result of government routine testing, none had taken voluntary testing. On COVID-19 vaccine, 36.8% of the respondents had information that teachers in public and private schools are a prioritized group for vaccination by the government against COVID-19. Of the sampled teachers, 92.4 % agreed that they needed more information on COVID-19 vaccine to make informed decision on vaccination. When asked “Who would you suggest to be the lead awareness campaigner on COVID-19 vaccine information to teachers” 93.2% of the teachers suggested officials from the Teachers Service Commission (TSC) working together with those from the Ministry of Education (MoE) to be the lead campaigners of COVID-19 vaccine awareness. Only 2.6 % and 1.1 % suggested TSC and MoE to lead the awareness on the vaccine respectively as separate government agencies. When respondents were asked if they would agree to be vaccinated against COVID-19 with a vaccine proven safe by the government, 34.7 % agreed that they would accept to be vaccinated. COVID-19 vaccine acceptance was strongly associated with gender and level of education. Both male and female primary certificate and diploma holders were more likely (PË0.05) to accept to be vaccinated compared to teachers whose highest level of education was a degree. However, the association between the vaccine acceptance among certificate and diploma holders was not significant (PË0.05) (Figure 1).
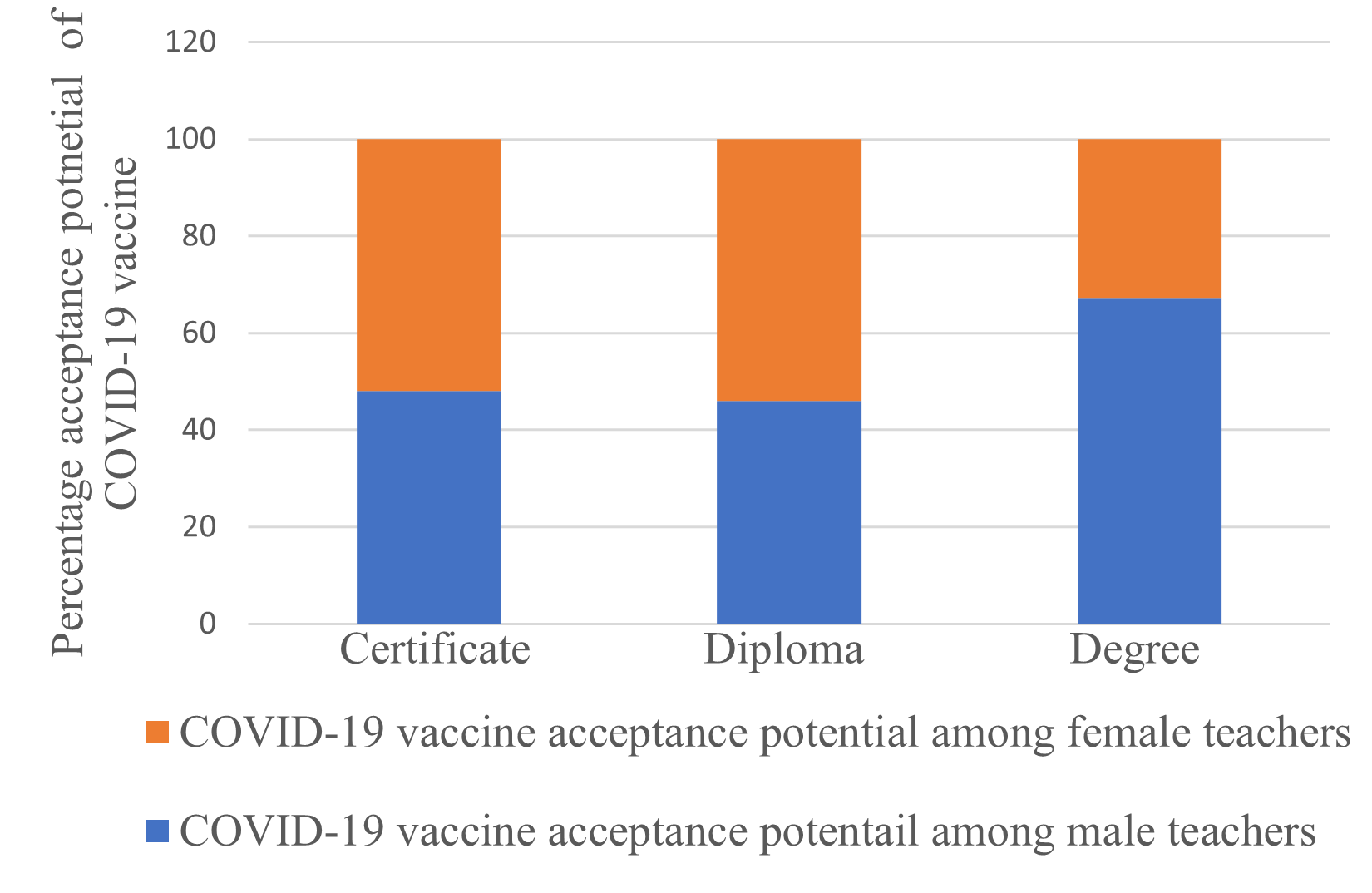
Figure 1: COVID-19 vaccine acceptance potential level among teachers. Among the sampled, 34.7 % of teachers agreed they would accept to be vaccinated with a safe COVID -19 vaccine. Male and female certificate and diploma teachers were more likely (PË0.05) to accept to be vaccinated against COVID-19 than teachers holding degrees. However, the association between COVID-19 vaccine acceptance among certificate and diploma teachers was not strong (PË0.05).
Of the respondents, 44.7 % disagreed to accept to be vaccinated while 20.5 % remained neutral on the COVID-19 vaccination acceptance. Asked whether they believed on safety of COVID-19 vaccine based on information they had, only 12.9 % of the respondents agreed that the vaccine is safe while, 40.8 % disagreed and 46.3 % remained neutral. The responses on the vaccine safety were statistically dependent on number of years in the teaching service and age group. Teachers aged between 23-35 years and whose teaching experience was between 0-5 years, and those aged between 46-59 years with teaching experience spanning 11-20 years and above, substantially (PË0.05) disagreed that the COVID-19 vaccine was safe compared to teachers within the age group of 36-45 years and whose teaching experience was between 6-10 years (Figure 2).
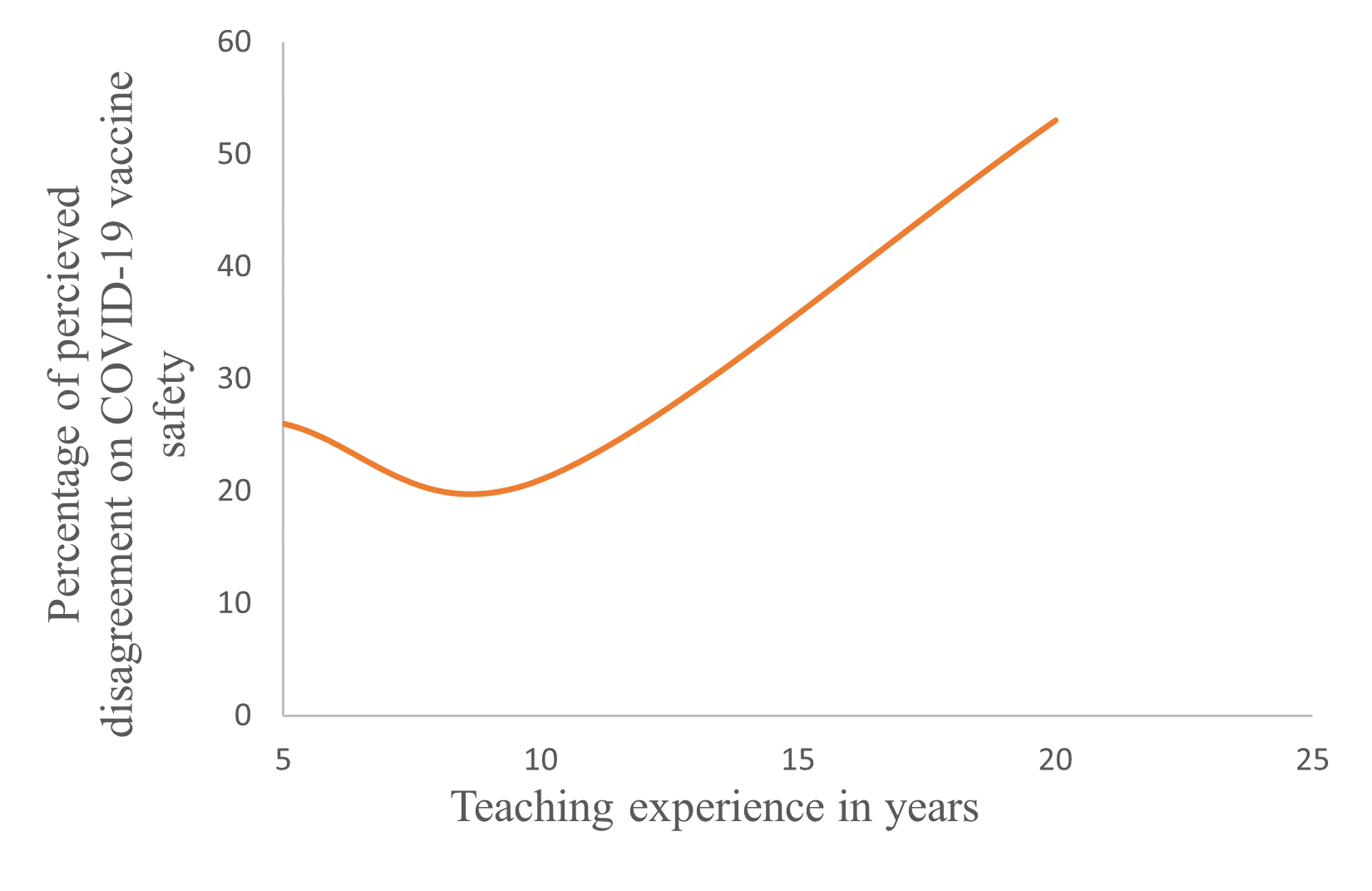
Figure 2: Relationship between teaching experience and perceived COVID-19 vaccine safety among teachers. Teachers whose teaching experience was between 0-5 years and 11-20 years substantially (PË0.05) disagreed that the COVID-19 vaccine was safe compared to those whose teaching experience was 6 -10 years.
Discussion
This is the first study to examine potential COVID-19 vaccine acceptance among teachers in Kenya. The data clearly indicates that teachers have basic information regarding the coronavirus disease 2019 but there is lack of sufficient information on the COVID-19 vaccine. Dearth of information on COVID-19 vaccine is likely to be a major obstacle in acceptance of the vaccine among teachers. The acceptance rate of 34.7 % is too low to achieve the desired level of vaccination among teachers in order to reduce risk of COVID-19 transmission in schools and in communities where teachers and learners are drawn from. The SAGE roadmap on sequential distribution of the COVID-19 approved vaccines recommends that, among the targeted, teachers in primary schools should be prioritized for COVID-19 vaccination because they face elevated risk of the disease transmission occasioned by inability to effectively physically keep distance from their learners. Additionally, the Kenya Basic Education COVID-19 Emergency Response Plan identified high learner congestion in primary schools as a potential risk for COVID-19 transmission. Among the sampled, 52 % were primary school teachers forming the largest proportion of the respondents. The government, therefore, should seize the opportunity presented by the high acceptance potential for the COVID-19 vaccine among the primary certificate and diploma teachers as indicated in this study. Kenyan government and other public health providers including Non-Governmental-Organizations such as the Red Cross and World Vision, which are present in the sub counties under the study, need to sensitize teachers on age related conditions that have been associated with severe forms of COVID-19 illness. Conditions such as diabetes, hypertension, asthma, overweight and being aged, inter lia, have been linked to severe COVID-19 illness13,14. Paradoxically, teachers in advanced age (46-59 years), expressed disagreement on the COVID-19 vaccine safety yet they formed the largest proportion of interviewees at 56 % of the sampled respondents. This group of teachers pose a serious threat on COVID-19 transmission both in school and within their communities of residence as has been observed in various studies15, and, therefore, they present a unique group who should be well informed on the benefits of the COVID-19 vaccines. Respondents suggested that a joint approach by the TSC and MoE officials would be the best in sensitizing teachers on COVID-19 vaccine information. This finding is consistent with that of Lazarus et al who, in a global survey of potential acceptance of a COVID-19 vaccine, found that employed respondents preferred getting information on COVID-19 vaccine safety and effectiveness from their employers16. This probably implies that teachers have trust in information passed onto them jointly by their employer, the TSC, and the MoE. Lessons from previous infectious disease pandemics and public health emergencies indicate trusted sources of information are fundamental to disease control17.
Clear and coherent communication by government officials is critical to building public confidence in vaccine programs. This should include explaining how vaccines work, how they are designed and developed and who approves them for safety. Further, targeted groups for vaccinations may require information on how long it takes for one to get protected following vaccination and whether multiple vaccine doses are required to confer protection. This study had limitations. The study was conducted at a time when the AstraZeneca vaccine had not yet been delivered in Kenya but at a time the vaccine had been withdrawn in South Africa for being unable to protect against a severe acute respiratory syndrome corona virus 2 (SARS-COV 2) variant in South Africa18. The low efficacy of the vaccine in South Africa may have changed teachers perceptive on the vaccine safety and effectiveness in Kenya. In order to improve trust among the teachers, the elements that define and help build trust should be well understood and interventions crafted appropriately. Transparent, evidence-informed policy and accurate yet clear communication will be required in increasing vaccine acceptance among teachers. Data presented in this study provides Kenyan public health providers with an opportunity to build vaccine literacy among teachers and instill confidence to support uptake of the approved COVID-19 vaccines, as well as bolster overall immunization for all vaccine-preventable diseases.
Declarations
Competing interests
The authors declare that they have no competing interests
Funding
Louise Bowditch provided funds for this research project
Author’s contributions
All authors: Contributed to conception, design, analysis and/or interpretation of the data
participated in drafting the article and revising the draft manuscript
Approved the final version of the manuscript for submission
Acknowledgment
We remain indebted to Louise Bowditch for providing funding for this study.
References
- Karafillakis E, Larson HJ. The benefit of the doubts or doubts over benefits? A systematic literature review of perceived risks of vaccines in European populations. Vaccine. 2017; 35, 4840-4850.
- Munoz CD, Llamas ML, Capblanch BX. Exposing concerns about vaccination in low-and middle-income countries: a systematic review. International Journal of Public Health. 2015; 60, 767-780.
- Li AJ, Tabu C, Shendale S, et al. Qualitative insights into reasons for missed opportunities for vaccination in Kenyan health facilities. PloS ONE. 2020; 15(3).
- Larson HJ, Jarrett C, Eckersberger E, et al. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systemic review of published literature, 2007-2012. Vaccine. 2014; 32, 2150-2159.
- Lane S, MacDonald NE, Marti M, et al. Vaccinehesitancy around the globe: analysis of three years of WHO/UNICEF joint Reporting Form data-2015-2017. Vaccine. 2018; 36, 3861-3867.
- Reuters News, 2020.
- Unite Nations Policy Brief, 2020.
- Ngwacho A. COVID-19 Pandemic Impact on Kenyan Education Sector: Learner Challenges and Mitigations. Journal of Research Innovation and Implications in Education 4. 2020; 128-139.
- Kenya Basic Education COVID-19 Emergency Response Plan, 2020.
- WorldMeter, 2020.
- Corona Vaccine Tracker, 2021.
- WHO SAGE Roadmap for prioritizing uses of COVID-19 Vaccines in the context of limited supply; 2020.
- Rita R.K, Sherita HG, William TC. Diabetes and Aging: Unique Considerations and Goals of Care. Diabetes Care. 2017; 40, 440-443.
- Christopher EC, Sinead TJM, Richard JM, et al. COVID-19 and hypertension: risks and management. A scientific statement on behalf of the British and Irish Hypertension Society. Journal of Human Hypertension. //doi.org/10.1038/s41371-020-0045-x, 2021
- Nicholas GD, Petra K, Yang L, et al. Age-dependent effects in the transmission and control of COVID-19 epidemics. Nature Medicine. 2020; 26, 1205-1211.
- Lazarus VJ, Scott CR, Adam P, et al. A global survey of potential acceptance of COVID-19 vaccine. 2020; Nature Medicine //doi.org/10.1038/s41591-020-1124-9,2020
- Siegrist M, Zingg A. The role of public trust during pandemics: implications for crisis communication. European Journal of Applied Physiology. 2014; 19, 23-32.
- Mancini DP, Kuchler H, Pilling D, et al. Oxford/AstraZeneca Jab fails to prevent mild and moderate COVID from South African strain. Financial Times. Feb 7, 2021.